

Possible Helpers in the Fight against COV-2, Explained
Saturday, March 21st, 2020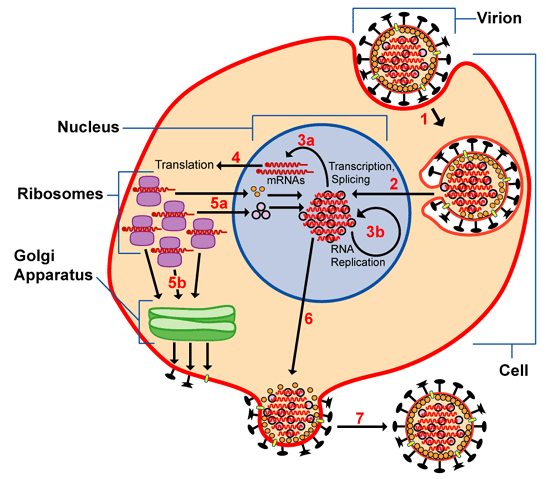
Image: RNA virus life cycle (NIH image via Wikipedia; Creative Commons)
{kind=link}
COV-2 is an RNA virus whose surface glycoprotein attaches to cell receptor ACE2 (angiotensin-converting enzyme-2, a regulator of heart and kidney function). COV-2 is a close relative of SARS and MERS, with bats as its primary reservoir. The fact that it’s an RNA virus means that it can mutate rapidly; other RNA viruses include hepatitis C, Ebola, HIV, polio, and influenza. COV-2 already has two variants. Not surprisingly, the most recent one causes higher lethality.
There are three potential treatments in train to help stem the COV-2 avalanche that’s now paralyzing our world. The main catch: to work, each has to be administered before people go into respiratory arrest or cytokine storm. My brief, lay summation of each potential therapeutic path follows. Please bear in mind that this is a rapidly evolving topic, and my earnest hope is that a vaccine soon gets added to the list.
1. Remdesivir, an adenosine analog that gets used by viral RNA polymerases, short-circuiting viral replication. Remdesivir was originally developed to treat Ebola, Marburg & MERS — and it does, though less efficiently than competitors. From these clinical trials, it’s known to be non-toxic, and the COV-2 polymerase is close enough to its original targets to be successfully decoyed. Because human RNA polymerases differ significantly from their viral equivalents, this treatment is likely to have low side effects.
2. Losartan and its relatives, anti-hypertensives that bind to the same cell surface receptor co-opted by COV-2. A known entity with established dosage and relatively low-key side effects, it exists as a generic. One major shortcoming is that it cannot be taken during pregnancy.
3. (Hydroxy)chloroquine, a well-established anti-malarial also used for lupus and arthritis, which blocks the release of viral RNA into host cells. As with losartan, it’s well-established but has some alarming side effects: cardiac arrhythmia that can be lethal (which means doses must be carefully calibrated according to weight), permanent retinal damage (increased chances if used long-term). The side effects have made compliance difficult even for people with malaria, but this would not be a barrier with COV-2 emergency treatment.
At this point, some US hospitals are already using Remdesivir and chloroquine, and the NIH has started expedited trials. I suspect the hospitals are not doing double-blind studies, because they’re faced with real life-and-death decisions. The true picture of efficacy, side effects, correct dosage, etc. will emerge from the NIH and its equivalents across the world, and it will take time. Where saving lives is involved, doctors at ground zero may have to opt for rapid non-guaranteed deployment of whatever promises to work.
ETA: a reader has also mentioned favipiravir, a synthetic molecule that disrupts the function of viral RNA polymerase. Favipiravir has shown promise equal to that of remdesivir in preliminary sallies.
Sites with important information:
National Institutes of Health (NIH)
Johns Hopkins
Centers for Disease Control (CDC)